Remedy For Bursitis Of The Foot
Overview
Bursitis is defined as inflammation of a bursa. Humans have approximately 160 bursae. These are saclike structures between skin and bone or between tendons, ligaments, and bone. The bursae are lined by synovial tissue, which produces fluid that lubricates and reduces friction between these structures.
Causes
Overusing your calves, ankles and heels during inappropriate or excessive training or doing repetitive motions for prolonged periods of time can contribute to the development of the this painful ankle Achilles and retrocalcaneal bursitis aliment. Bursitis in this part of the body often occurs in professional or recreational athletes. Walking, running and jumping can do some damage. (I loved to skip rope before I suffered my severe hip bursitis.). Injury. This condition may also develop following trauma such as a direct, hard hit to your heel. Footwear. Poorly fitting shoes that are too tight, too large or have heels can all cause excessive pressure or friction over the bursa in the heel. Infection. Medical problems, such as rheumatoid arthritis or gout, sometimes lead to bursitis. It is not unusual to have Achilles bursitis and tendonitis (inflamed tendon) at the same time. Ankle bursitis is often a genetic condition where you simply inherited a foot type, for example a heel bone with a prominence, high arch or tight Achilles tendon, that is more prone to the mechanical irritation that leads to the bursitis. Muscle weakness, joint stiffness and poor flexibility (particularly of the calf muscles) are certainly contributing factors too.
Symptoms
Pain at the back of the heel at the attachment site of the Achilles tendon when running. Pain on palpation of the back of the heel or bottom of heel. Pain when standing on tiptoes. Swelling and redness at the back and bottom of the heel.
Diagnosis
Diagnosis of heel bursitis can be made by your health practitioner and is based on the following. Assessing the location of the pain by palpating the back of the heel. Assessment of any inflammation at the back of the heel. Assessment of biomechanics and foot function. Ultrasound or MRI can reveal inflammation of the retro calcaneal bursa.
Non Surgical Treatment
Home treatment is often enough to reduce pain and let the bursa heal. Your doctor may suggest physical therapy to strengthen the muscles around your joints. Rest the affected area. Avoid any activity or direct pressure that may cause pain. Apply ice or cold packs as soon as you notice pain in your muscles or near a joint. Apply ice 10 to 15 minutes at a time, as often as twice an hour, for 3 days (72 hours). You can try heat, or alternating heat and ice, after the first 72 hours. Use pain relievers. Use nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, to reduce pain and inflammation. NSAIDs come in pills and also in a cream that you rub over the sore area. Acetaminophen (such as Tylenol) can also help with pain. Don't rely on medicine to relieve pain so that you can keep overusing the joint. Do range-of-motion exercises each day. If your bursitis is in or near a joint, gently move the joint through its full range of motion, even during the time that you are resting the joint area. This will prevent stiffness. As the pain goes away, add other exercises to strengthen the muscles around your joint. Avoid tobacco smoke.Smoking delays wound and tissue healing. If you have severe bursitis, your doctor may use a needle to remove extra fluid from the bursa. You might wear a pressure bandage on the area. Your doctor may also give you a shot of medicine to reduce swelling. Some people need surgery to drain or remove the bursa. Sometimes the fluid in the bursa can get infected. If this happens, you may need antibiotics. Bursitis is likely to improve in a few days or weeks if you rest and treat the affected area. But it may return if you don't stretch and strengthen the muscles around the joint and change the way you do some activities.
Prevention
Continue to wear your orthotics for work and exercise to provide stability and restore foot function. Select suitable shoes for work and physical activity that provide stability for the heel. Regular stretching of the calf muscle can prevent heel bursitis. Do not suddenly increase activity amount without appropriate conditioning.
Bursitis is defined as inflammation of a bursa. Humans have approximately 160 bursae. These are saclike structures between skin and bone or between tendons, ligaments, and bone. The bursae are lined by synovial tissue, which produces fluid that lubricates and reduces friction between these structures.
Causes
Overusing your calves, ankles and heels during inappropriate or excessive training or doing repetitive motions for prolonged periods of time can contribute to the development of the this painful ankle Achilles and retrocalcaneal bursitis aliment. Bursitis in this part of the body often occurs in professional or recreational athletes. Walking, running and jumping can do some damage. (I loved to skip rope before I suffered my severe hip bursitis.). Injury. This condition may also develop following trauma such as a direct, hard hit to your heel. Footwear. Poorly fitting shoes that are too tight, too large or have heels can all cause excessive pressure or friction over the bursa in the heel. Infection. Medical problems, such as rheumatoid arthritis or gout, sometimes lead to bursitis. It is not unusual to have Achilles bursitis and tendonitis (inflamed tendon) at the same time. Ankle bursitis is often a genetic condition where you simply inherited a foot type, for example a heel bone with a prominence, high arch or tight Achilles tendon, that is more prone to the mechanical irritation that leads to the bursitis. Muscle weakness, joint stiffness and poor flexibility (particularly of the calf muscles) are certainly contributing factors too.
Symptoms
Pain at the back of the heel at the attachment site of the Achilles tendon when running. Pain on palpation of the back of the heel or bottom of heel. Pain when standing on tiptoes. Swelling and redness at the back and bottom of the heel.
Diagnosis
Diagnosis of heel bursitis can be made by your health practitioner and is based on the following. Assessing the location of the pain by palpating the back of the heel. Assessment of any inflammation at the back of the heel. Assessment of biomechanics and foot function. Ultrasound or MRI can reveal inflammation of the retro calcaneal bursa.
Non Surgical Treatment
Home treatment is often enough to reduce pain and let the bursa heal. Your doctor may suggest physical therapy to strengthen the muscles around your joints. Rest the affected area. Avoid any activity or direct pressure that may cause pain. Apply ice or cold packs as soon as you notice pain in your muscles or near a joint. Apply ice 10 to 15 minutes at a time, as often as twice an hour, for 3 days (72 hours). You can try heat, or alternating heat and ice, after the first 72 hours. Use pain relievers. Use nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen, to reduce pain and inflammation. NSAIDs come in pills and also in a cream that you rub over the sore area. Acetaminophen (such as Tylenol) can also help with pain. Don't rely on medicine to relieve pain so that you can keep overusing the joint. Do range-of-motion exercises each day. If your bursitis is in or near a joint, gently move the joint through its full range of motion, even during the time that you are resting the joint area. This will prevent stiffness. As the pain goes away, add other exercises to strengthen the muscles around your joint. Avoid tobacco smoke.Smoking delays wound and tissue healing. If you have severe bursitis, your doctor may use a needle to remove extra fluid from the bursa. You might wear a pressure bandage on the area. Your doctor may also give you a shot of medicine to reduce swelling. Some people need surgery to drain or remove the bursa. Sometimes the fluid in the bursa can get infected. If this happens, you may need antibiotics. Bursitis is likely to improve in a few days or weeks if you rest and treat the affected area. But it may return if you don't stretch and strengthen the muscles around the joint and change the way you do some activities.
Prevention
Continue to wear your orthotics for work and exercise to provide stability and restore foot function. Select suitable shoes for work and physical activity that provide stability for the heel. Regular stretching of the calf muscle can prevent heel bursitis. Do not suddenly increase activity amount without appropriate conditioning.
Is A Hammer Toe Uncomfortable
 Overview
Overview
A hammertoe is a contracture-or bending-of the toe at the first joint of the digit, called the proximal interphalangeal joint. This bending causes the toe to appear like an upside-down V when looked at from the side. Any toe can be involved, but the condition usually affects the second through fifth toes, known as the lesser digits. Hammertoes are more common to females than males.
Causes
A person may be born with hammer toe or may develop it from wearing short, narrow shoes. Hammer toe can occur in children who outgrow shoes rapidly. Sometimes hammer toe is genetic and is caused by a nerve disorder in the foot. High heeled shoes are can also cause hammer toe. The reason for this is that the toes are not only bunched up, but the weight of the body is pushing them forward even further.
 Symptoms
Symptoms
Hammer toe is often distinguished Hammer toes by a toe stuck in an upside-down ?V? position, and common symptoms include corns on the top of your toe joint. Pain at the top of a bent toe when you put on your shoes. Pain when moving a toe joint. Pain on the ball of your foot under the bent toe. Corns developing on the top of the toe joint. It is advisable to seek medical advice if your feet hurt on a regular basis. It is imperative to act fast and seek the care of a podiatrist or foot surgeon. By acting quickly, you can prevent your problem from getting worse.
Diagnosis
The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position.
Non Surgical Treatment
Orthotics are shoe inserts that can help correct mechanical foot-motion problems to correct pressure on your toe or toes and reduce pain. Changing shoes. You should seek out shoes that conform to the shape of your feet as much as possible and provide plenty of room in the toe box, ensuring that your toes are not pinched or squeezed. You should make sure that, while standing, there is a half inch of space for your longest toe at the end of each shoe. Make sure the ball of your foot fits comfortably in the widest part of the shoe. Feet normally swell during the course of the day, so shop for shoes at the end of the day, when your feet are at their largest. Don't be vain about your shoe size, sizes vary by brand, so concentrate on making certain your shoes are comfortable. Remember that your two feet are very likely to be different sizes and fit your shoe size to the larger foot. Low-heel shoes. High heels shift all your body weight onto your toes, tremendously increasing the pressure on them and the joints associated with them. Instead, wear shoes with low (less than two inches) or flat heels that fit your foot comfortably.
Surgical Treatment
Surgical correction is needed to bring the toe into a corrected position and increase its function. Correction of the hammer toes is a simple outpatient surgery, with limited downtime. The best option is to fuse the deformed and contracted toe into a straight position. This limits the need for future surgery and deformity return. A new pin that absorbs in the bone or small screw is used by the Foot and Ankle Institute to avoid the need for a metal pin protruding from the toe during recovery. Although the absorbable pin is not for everyone, it is much more comfortable than the pin protruding from the end of the toe. In certain cases, a removal of a small area of bone in the deformity area will decrease pain and limit the need for a surgical waiting period that is found with fusions. Although the toe is not as stable as with a fusion, in certain cases, an arthroplasty is the best option.
Over-Pronation
Overview
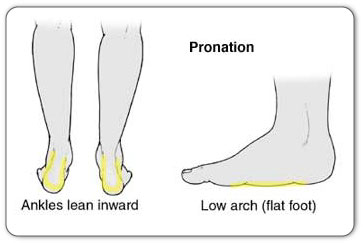
Simply put, over-pronation is an excessive or poorly timed pronation which is part of the regular stride. Pronation is when the foot rolls inwards and the arch compresses as part of your normal walking motion. Pronation is necessary for shock absorption to transmit forces up and down our legs. When someone over-pronates, the foot rolls inwards to a greater degree and the arch flattens: this causes the knee and hip to come out of alignment and reduces the function of all the bones in the feet.
Causes
In adults, the most common reason for the onset of Over-Pronation is a condition known as Post Tibial Tendonitis. This condition develops from repetitive stress on the main supporting tendon (Posterior Tibial Tendon) of the foot arch. As the body ages, ligaments and muscles can weaken. When this occurs the job of providing the majority of the support required by the foot arch is placed upon this tendon. Unfortunately, this tendon cannot bear the weight of this burden for too long. Eventually it fatigues under the added strain and in doing so the foot arch becomes progressively lower over a period of time.
Symptoms
If you overpronate, your symptoms may include discomfort in the arch and sole of foot, your foot may appear to turn outward at the ankle, your shoes wear down faster on the medial (inner) side of your shoes. Pain in ankle, shins, knees, or hips, especially when walking or running are classic symptoms of overpronation. Overpronation can lead to additional problems with your feet, ankles, and knees. Runners in particular find that overpronation can lead to shin splints, tarsal tunnel syndrome, plantar fasciitis, compartment syndrome, achilles tendonitis, bunions or hallux valgus, patello-femoral pain syndrome, heel spurs, metatarsalgia.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Simply put, over-pronation is an excessive or poorly timed pronation which is part of the regular stride. Pronation is when the foot rolls inwards and the arch compresses as part of your normal walking motion. Pronation is necessary for shock absorption to transmit forces up and down our legs. When someone over-pronates, the foot rolls inwards to a greater degree and the arch flattens: this causes the knee and hip to come out of alignment and reduces the function of all the bones in the feet.
Causes
In adults, the most common reason for the onset of Over-Pronation is a condition known as Post Tibial Tendonitis. This condition develops from repetitive stress on the main supporting tendon (Posterior Tibial Tendon) of the foot arch. As the body ages, ligaments and muscles can weaken. When this occurs the job of providing the majority of the support required by the foot arch is placed upon this tendon. Unfortunately, this tendon cannot bear the weight of this burden for too long. Eventually it fatigues under the added strain and in doing so the foot arch becomes progressively lower over a period of time.
Symptoms
If you overpronate, your symptoms may include discomfort in the arch and sole of foot, your foot may appear to turn outward at the ankle, your shoes wear down faster on the medial (inner) side of your shoes. Pain in ankle, shins, knees, or hips, especially when walking or running are classic symptoms of overpronation. Overpronation can lead to additional problems with your feet, ankles, and knees. Runners in particular find that overpronation can lead to shin splints, tarsal tunnel syndrome, plantar fasciitis, compartment syndrome, achilles tendonitis, bunions or hallux valgus, patello-femoral pain syndrome, heel spurs, metatarsalgia.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Addressing Severs Disease
Overview
Sever condition is an inflammation of the growth plate of the bone at the back of the heel (apophysitis of the calcaneus). The inflammation of Sever condition is at the point where the Achilles tendon attaches to the back of the heel bone. What causes Sever condition? Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Causes
Sever?s disease is common, and typically occurs during a child?s growth spurt, which can occur between the ages of 10 and 15 in boys and between the ages of 8 and 13 in girls. Feet tend to grow more quickly than other parts of the body, and in most kids the heel has finished growing by the age of 15. Being active in sports or participating in an activity that requires standing for long periods can increase the risk of developing Sever?s disease. In some cases, Sever?s disease first becomes apparent after a child begins a new sport, or when a new sports season starts. Sports that are commonly associated with Sever?s disease include track, basketball, soccer, and gymnastics. Children who are overweight or obese are also at a greater risk of developing this condition. Certain foot problems can also increase the risk, including. Over pronating. Kids who over pronate (roll the foot inward) when walking may develop Sever?s disease. Flat foot or high arch. An arch that is too high or too low can put more stress on the foot and the heel, and increase the risk of Sever?s disease. Short leg. Children who have one leg that is shorter than the other may experience Sever?s disease in the foot of the shorter leg because that foot is under more stress when walking.
Symptoms
Chief complaint is heel pain which increases pain during running and jumping activities. Pain is localized to the very posterior aspect of the heel. Pain is elicited only with weightbearing. Mild involvement is present if pain is brought on only with running during sports. The symptoms can be severe, with pain (and possibly limp) with activities of daily living (ie walking).
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
In general, the goals for treatment include reducing the localized areas of inflammation. We recommend that patients utilize Ibuprofen every six to eight hours as needed. Stretching exercises on a daily basis, as well as prior to activity is thought to be helpful as well. Following work-outs and increased activities, it may be helpful to apply ice over affected areas. Heel cups are also available to provide cushion in shoes. In addition, for more severe symptoms, it may be helpful to refrain from sports and/or immobilize the area for a few weeks to help reduce the inflammation.
Prevention
The best way to prevent Sever?s disease is for your child to stay flexible and stretch the hamstring, calf muscles, and the Achilles tendon before and after activity each day. It?s important to hold the stretches for 20 seconds and stretch both legs, even if there is only pain in one. If he or she only has smaller symptoms, like swelling and some tenderness, consider your child lucky. They may only have to sit out for one to two weeks during the season. The best treatment is to immediately stop the activity that caused the pain. Elevate and ice the heel for 20 minutes at a time to relieve discomfort and swelling.
Sever condition is an inflammation of the growth plate of the bone at the back of the heel (apophysitis of the calcaneus). The inflammation of Sever condition is at the point where the Achilles tendon attaches to the back of the heel bone. What causes Sever condition? Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Causes
Sever?s disease is common, and typically occurs during a child?s growth spurt, which can occur between the ages of 10 and 15 in boys and between the ages of 8 and 13 in girls. Feet tend to grow more quickly than other parts of the body, and in most kids the heel has finished growing by the age of 15. Being active in sports or participating in an activity that requires standing for long periods can increase the risk of developing Sever?s disease. In some cases, Sever?s disease first becomes apparent after a child begins a new sport, or when a new sports season starts. Sports that are commonly associated with Sever?s disease include track, basketball, soccer, and gymnastics. Children who are overweight or obese are also at a greater risk of developing this condition. Certain foot problems can also increase the risk, including. Over pronating. Kids who over pronate (roll the foot inward) when walking may develop Sever?s disease. Flat foot or high arch. An arch that is too high or too low can put more stress on the foot and the heel, and increase the risk of Sever?s disease. Short leg. Children who have one leg that is shorter than the other may experience Sever?s disease in the foot of the shorter leg because that foot is under more stress when walking.
Symptoms
Chief complaint is heel pain which increases pain during running and jumping activities. Pain is localized to the very posterior aspect of the heel. Pain is elicited only with weightbearing. Mild involvement is present if pain is brought on only with running during sports. The symptoms can be severe, with pain (and possibly limp) with activities of daily living (ie walking).
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
In general, the goals for treatment include reducing the localized areas of inflammation. We recommend that patients utilize Ibuprofen every six to eight hours as needed. Stretching exercises on a daily basis, as well as prior to activity is thought to be helpful as well. Following work-outs and increased activities, it may be helpful to apply ice over affected areas. Heel cups are also available to provide cushion in shoes. In addition, for more severe symptoms, it may be helpful to refrain from sports and/or immobilize the area for a few weeks to help reduce the inflammation.
Prevention
The best way to prevent Sever?s disease is for your child to stay flexible and stretch the hamstring, calf muscles, and the Achilles tendon before and after activity each day. It?s important to hold the stretches for 20 seconds and stretch both legs, even if there is only pain in one. If he or she only has smaller symptoms, like swelling and some tenderness, consider your child lucky. They may only have to sit out for one to two weeks during the season. The best treatment is to immediately stop the activity that caused the pain. Elevate and ice the heel for 20 minutes at a time to relieve discomfort and swelling.
Achilles Tendon Rupture Recovery Complications
Overview
 An Achilles Tendon Rupture is a traumatic event that needs appropriate treatment by your physician. The rupture can either be partial or complete depending on the severity. A thorough evaluation needs to be made to differentiate a tendonitis from a rupture and to evaluate the extent of the rupture.
An Achilles Tendon Rupture is a traumatic event that needs appropriate treatment by your physician. The rupture can either be partial or complete depending on the severity. A thorough evaluation needs to be made to differentiate a tendonitis from a rupture and to evaluate the extent of the rupture.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are corticosteroid medication (such as prednisolone), mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing?s syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture, for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE) - lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked.
Diagnosis
To diagnose an Achilles tendon injury, your health care provider will give you a thorough physical exam. He or she may want to see you walk or run to look for problems that might have contributed to your Achilles tendon injury.
Non Surgical Treatment
You may need to wear a plaster cast, brace or boot on your lower leg for six to eight weeks to help the tendon heal. During this time, your doctor will change the cast a number of times to make sure your tendon heals in the right way. If your tendon is partially ruptured, your doctor will probably advise you to have this treatment instead of surgery. It?s also suitable for people who aren't very physically active. However, there is a greater risk that your tendon will rupture again, compared with surgery. Your doctor will advise you which treatment is best for you. 
Surgical Treatment
Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
Rigid Flat Feet In Adults
Overview
Adult-Acquired Flat Foot Deformity (AAFFD) is most commonly caused by a progressive degeneration of the tendon (tibialis posterior) that supports the arch of the foot. As the tendon ages or is subjected to repetitive trauma, it stretches out over time, the natural arch of the foot becomes less pronounced and the foot gradually flattens out. Although it is uncertain why this occurs, the problem is seen equally among men and women - at an increasing frequency with age. Occasionally, a patient will experience a traumatic form of the condition as a result of a fall from a height or abnormal landing during aerial sports such as gymnastics or basketball. 
Causes
Adult flatfoot typically occurs very gradually. If often develops in an obese person who already has somewhat flat feet. As the person ages, the tendons and ligaments that support the foot begin to lose their strength and elasticity.
Symptoms
Symptoms of pain may have developed gradually as result of overuse or they may be traced to one minor injury. Typically, the pain localizes to the inside (medial) aspect of the ankle, under the medial malleolus. However, some patients will also experience pain over the outside (lateral) aspect of the hindfoot because of the displacement of the calcaneus impinging with the lateral malleolus. This usually occurs later in the course of the condition. Patients may walk with a limp or in advanced cases be disabled due to pain. They may also have noticed worsening of their flatfoot deformity.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
Non-surgical treatment includes rest and reducing your activity until the pain improves. Orthotics or bracing help support the tendon to reduce its pull along the arch, thus reducing pain. In moderate to severe cases, a below knee cast or walking boot may be needed to allow the tendon to rest completely and heal. Physical therapy is an integral part of the non-surgical treatment regimen to reduce inflammation and pain. Anti-inflammatory medication is often used as well. Many times evaluation of your current shoes is necessary to ensure you are wearing appropriate shoe gear to prevent re-injury. 
Surgical Treatment
A new type of surgery has been developed in which surgeons can re-construct the flat foot deformity and also the deltoid ligament using a tendon called the peroneus longus. A person is able to function fully without use of the peroneus longus but they can also be taken from deceased donors if needed. The new surgery was performed on four men and one woman. An improved alignment of the ankle was still evident nine years later, and all had good mobility 8 to 10 years after the surgery. None had developed arthritis.